Two events were crucial in the professionalization of surgery in America: Samuel Gross founded the American Surgical Association in 1880, and The Annals of Surgery—a journal devoted exclusively to surgery—was edited by Lewis Pilcher. The final stage of American surgical development occurred in May 1889 when William Halsted started working at the new John Hopkins University. He set the tone of surgery from the dramatic operating theatre to the more subdued operating room, while also emphasizing independent, original research and innovation.[53] With a dedicated medical school of surgery, surgical society, and a specialized surgical journal, American surgery became a real science[54].
Works Cited
“A Manual of Military Surgury.” Accessed October 29, 2017. http://jdc.jefferson.edu/cgi/viewcontent.cgi?article=1000&context=milsurgusa
Administration-1943, Farm Security. English: Johns Hopkins Hospital, Baltimore, Maryland. Operating Room (Reenacted). May 1943. http://memory.loc.gov/cgi-bin/query/D?fsaall:4:./temp/~ammem_Vc2n: https://commons.wikimedia.org/wiki/File:Johns_Hopkins_Hospital,_Baltimore,_Maryland.Operating_room(reenacted)..jpg
AfroBrazilian. English: Liston Bone Cutting Forcep Curved. [object HTMLTableCellElement]. Own work. https://commons.wikimedia.org/wiki/File:Liston_Bone_Cutting_Forcep_curved_01.jpg
“An Experimental and Critical Inquiry into the Nature and Treatment of Wounds of the Intestines.” Accessed October 29, 2017. https://collections.nlm.nih.gov/bookviewer?PID=nlm:nlmuid-65711820R-bk
“Broken Bodies, Suffering Spirits: Injury, Death, and Healing in Civil War Philadelphia.” Accessed February 2, 2019. http://muttermuseum.org/exhibitions/broken-bodies-suffering-spirits-injury-death-and-healing-in-civil-war-philadelphia/
Drexler, Madeline, and Institute of Medicine (US). How Infection Works. National Academies Press (US), 2010. https://www.ncbi.nlm.nih.gov/books/NBK209710/
Eakins, Thomas. Portrait of Dr. Samuel D. Gross (The Gross Clinic). 1875. Oil on canvasQS:P186,Q296955;P186,Q4259259,P518,Q861259, Height: 243.8 cm (95.9 in); Width: 198.1 cm (77.9 in) dimensions QS:P2048,243.8U174728;P2049,198.1U174728. Philadelphia Museum of Art. https://commons.wikimedia.org/wiki/File:EakinsTheGrossClinic.jpg
“Elements of Pathological Anatomy.” Accessed October 29, 2017. https://ia802604.us.archive.org/28/items/elementsofpathol01gros/elementsofpathol01gros.pdf
“File:The Medical and Surgical History of the War of the Rebellion. Part III, Volume II. (3rd Surgical Volume) (1883) (14759525401).Jpg - Wikimedia Commons.” Accessed October 28, 2017. https://commons.wikimedia.org/wiki/File:The_Medical_and_Surgical_History_of_the_War_of_the_Rebellion.Part_III,Volume_II.(3rd_Surgical_volume)(1883)_(14759525401).jpg
“Gas Gangrene: MedlinePlus Medical Encyclopedia.” Accessed October 28, 2017. https://medlineplus.gov/ency/article/000620.htm
“Gas_gangrene.Jpg (JPEG Image, 1200 × 960 Pixels).” Accessed October 28, 2017. https://upload.wikimedia.org/wikipedia/commons/8/81/Gas_gangrene.jpg
“Germ Theory.” Accessed October 29, 2017. http://broughttolife.sciencemuseum.org.uk/broughttolife/techniques/germtheory
Hager, Thomas. The Demon Under the Microscope: From Battlefield Hospitals to Nazi Labs, One Doctor’s Heroic Search for the World’s First Miracle Drug. Three Rivers Press, 2006
Internet Archive Book Images. Image from Page 37 of “Orthopaedic Surgery for Students and General Practitioners : Preliminary Considerations and Diseases of the Spine : 114 Original Illustrations” (1907). January 1, 1907. Photo. https://www.flickr.com/photos/internetarchivebookimages/14761163596/
Pitt, Dennis, and Jean-Michel Aubin. “Joseph Lister: Father of Modern Surgery.” Canadian Journal of Surgery 55, no. 5 (October 2012): E8–9. https://doi.org/10.1503/cjs.007112
Rutkow, Ira M. Surgery: An Illustrated History. Mosby-Year Book Incorporated in collaboration with Norman Pub, 1993.
Services, National Institutes of Health, Health & Human. Human Distal Femur Shot with a 510-Grain Lead Minié Ball Fired from a .58 Caliber Springfield Model 1862 Rifle. February 16, 2006. Leg bone from the Ragsdale Gunshot Wound Study, 1984. National Museum of Health and Medicine, Armed Forces Institute of Pathology, Washington, D.C. From exhibition “Visible Proofs: Forensic Views of the Body” U.S. National Library of Medicine, 8600 Rockville Pike, Bethesda, MD 20894. https://commons.wikimedia.org/wiki/File:Gunshot_femur.jpg
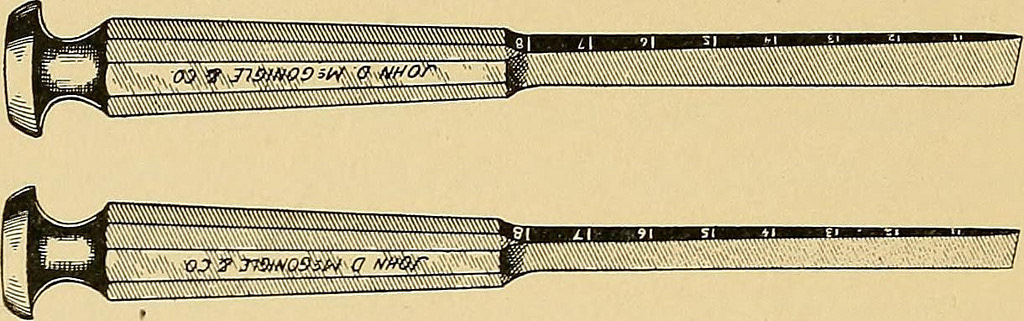
Set of Four Liston-Type Amputation Knives, London, England,. https://wellcomeimages.org/indexplus/obf_images/15/d2/6c762e237bd9f018c64157986cdb.jpg Gallery: https://wellcomeimages.org/indexplus/image/L0057237.html Wellcome Collection gallery (2018-04-02): https://wellcomecollection.org/works/r47dvbc9 CC-BY-4.0. Accessed August 14, 2018. https://commons.wikimedia.org/wiki/File:Set_of_four_Liston-type_amputation_knives,_London,_England,_Wellcome_L0057237.jpg
Society, Minnesota Historical. English: Artillery Shot-Canister for a 12-Pounder Cannon. The Canister Has a Wood Sabot, Iron Dividing Plate, and Thirty-Seven Cast-Iron Grape Shot. The Grapeshot All Have Mold-Seam Lines, and Some Have Sprue Projections. The Cylindrical Canister Has a Soldered Seam up One Side and Is Nailed to the Sabot, Which Is Cut with Two Encircling Grooves. A Second Plate inside the Canister Is Loose. An Iron Disc Divider Is Also Present. March 14, 2012. http://collections.mnhs.org/cms/display.php?irn=10430259&websites=no&brand=cms&q=civil%20war%20shot&startindex=1&count=25. https://commons.wikimedia.org/wiki/File:MHS_canister_shot.jpg
Stauch, Edward. Hospital Gangrene of an Arm Stump. 1863. [1]; also previously available at [2]; also a copy at Wallen.jpg described at “To Bind Up the Nation’s Wounds: Evacuation and Hospitalization” exhibit of the National Museum of Health and Medicine. https://commons.wikimedia.org/wiki/File:Wallen_wounded_by_Minie_ball.jpg
Surgical Instruments: Various Bullet Extractors. https://wellcomeimages.org/indexplus/obf_images/1b/c6/37a9648a6a8512d4216a3323a18f.jpg Gallery: https://wellcomeimages.org/indexplus/image/M0008371.html Wellcome Collection gallery (2018-04-03): https://wellcomecollection.org/works/kkjr69st CC-BY-4.0. Accessed August 14, 2018. https://commons.wikimedia.org/wiki/File:Surgical_Instruments;_various_bullet_extractors_Wellcome_M0008371.jpg
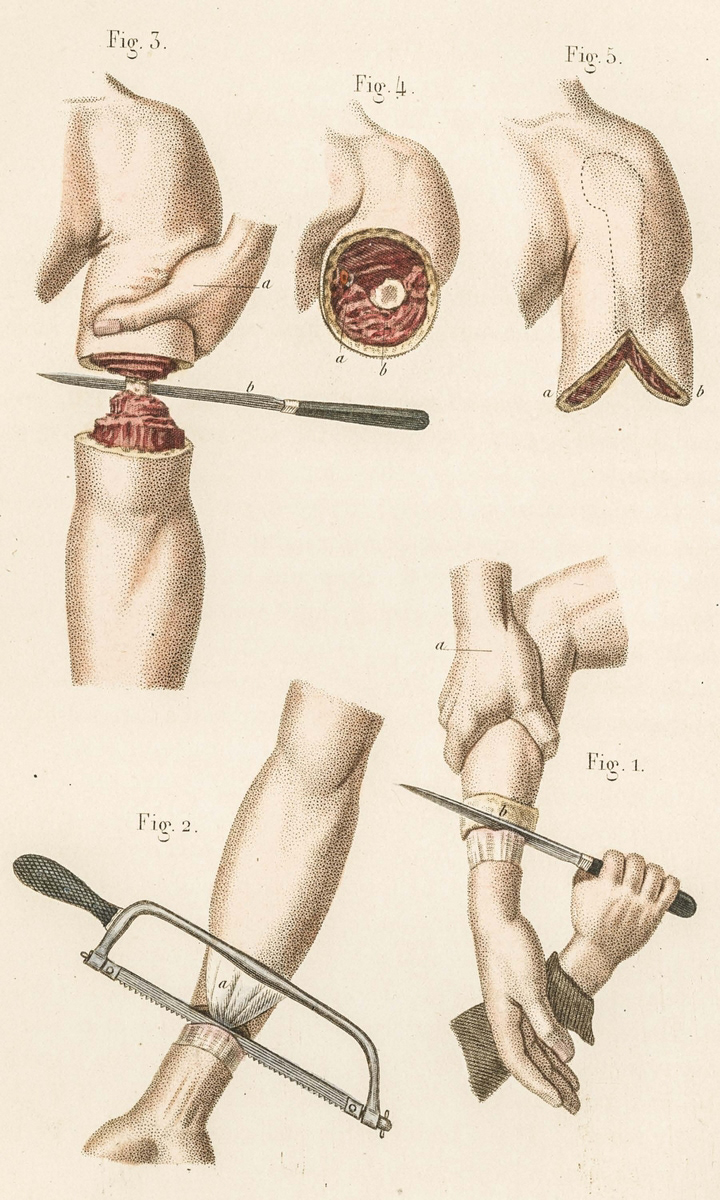
“Tools and Procedures for Amputation of the Arm.” Accessed August 10, 2021. https://www.cppdigitallibrary.org/items/show/4407
“The Rules of Aseptic and Antiseptic Surgery.” Accessed October 29, 2017. https://ia800708.us.archive.org/35/items/39002011127058.med.yale.edu/39002011127058.med.yale.edu.pdf
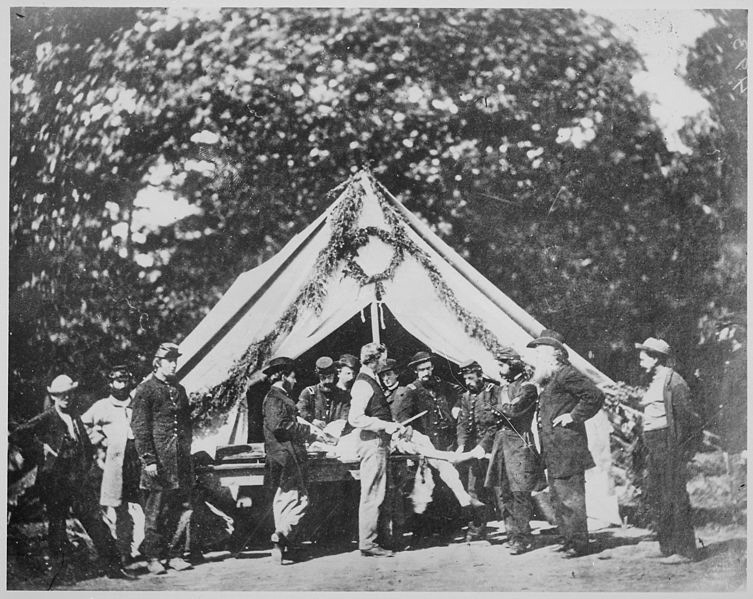
Tyson, Attributed to Charles J. Amputation Being Performed in a Hospital Tent, Gettysburg. July 1863. National Archives at College Park. https://commons.wikimedia.org/wiki/File:Amputation_being_performed_in_a_hospital_tent,_Gettysburg,07-1863-NARA-_520203.jpg
Unknown. English: Interior of Red Rover Civil War Hospital Steamship Published in Harper’s Weekly. January 2, 1863. Harper’s Weekly Illustration. https://commons.wikimedia.org/wiki/File:Interior_of_Red_Rover_Civil_War_hospital_steamship_published_in_Harper%27s_Weekly.png.
User:quadell. Civil War Surgeons Kit. August 10, 2013. Own work. https://commons.wikimedia.org/wiki/File:Civil_War_surgeons_kit.jpeg
USA, Laika ac from. 19th Century Bone Saw. October 12, 2013. 19th Century Bone Saw. https://commons.wikimedia.org/wiki/File:Laika_ac_19th_Century_Bone_Saw_(10441700906).jpg
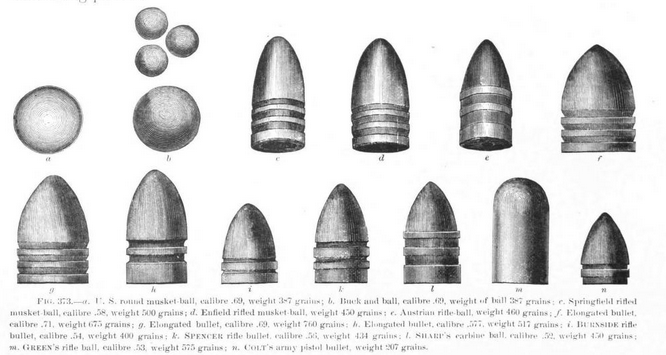
USG. English: Illustration from The Medical and Surgical History of the War of the Rebellion (USG Printing Office, 1870-88) - Various Projectiles during the American Civil War - Part III Vol 2. August 24, 2013. The Medical and Surgical History of the War of the Rebellion (US Gov’t Printing Office, 1870-88). https://commons.wikimedia.org/wiki/File:MSHWR_-_Projectiles_american_civil_war.png















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_(1883)_(14759525401).jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
..jpg){kind=link}